Grinding and Fatigue Acceleration
Lesson 23 · Structural Decision Framework
In plain English
We see this all the time: a 45-year-old patient cracks a back tooth that's never been touched. No fillings. No cavities ever on that tooth. They brush, they floss, they do everything right.
"How is this happening?"
The X-ray shows no decay. The bite check shows the answer: years of nighttime grinding the patient never knew they did. The tooth wasn't broken by something they did wrong, it was broken by something they did unconsciously, every night, for two decades.
Here's the part most patients don't realize:
Normal chewing isn't what wears teeth out fastest. Grinding is.
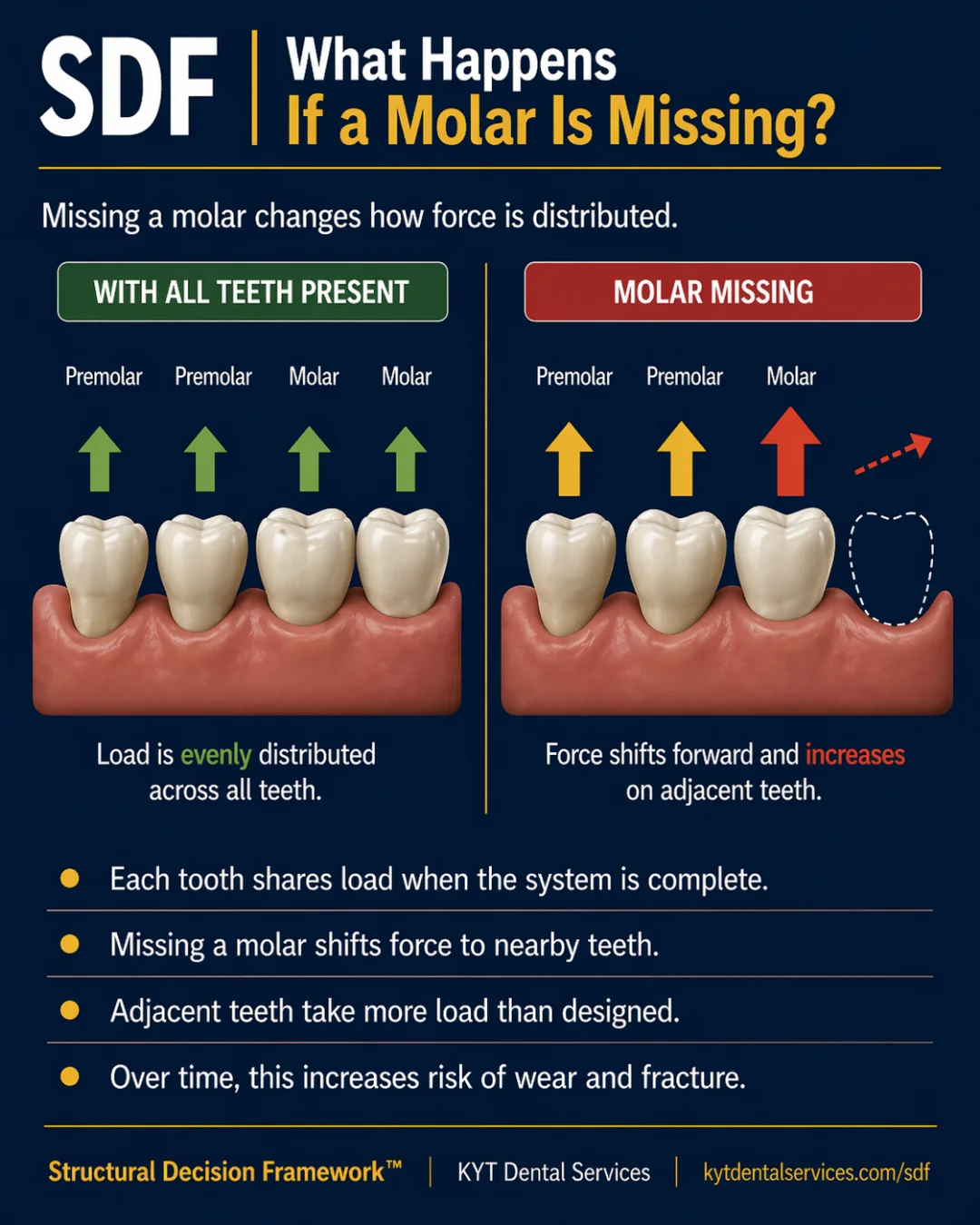
When you chew food, the force on your teeth is moderate and rhythmic, within what they were designed to absorb. Grinding is different. It produces force spikes far above the normal range, sometimes two to ten times higher, sustained for long periods, and most often happening during sleep when there's no conscious moderation.
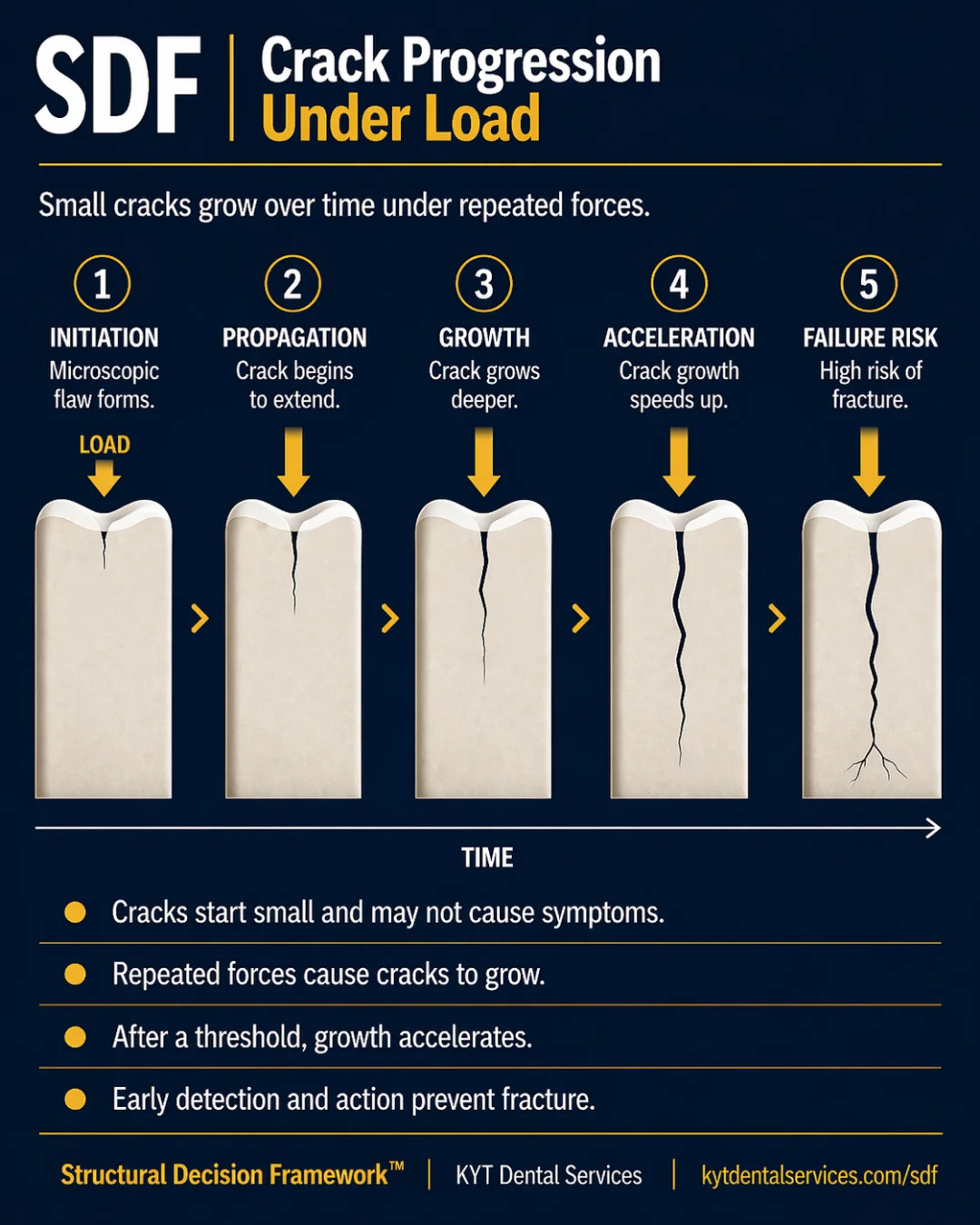
Each spike, on its own, doesn't break a tooth. What it does is leave a tiny bit of microdamage, a microcrack growing a fraction of a millimeter, a stress at a restoration margin, a cusp flexing past its limit. None of those are visible day-to-day. None of them hurt.
But fatigue accumulates the way it does in any material, invisible until it isn't. A grinder's mouth ages structurally faster than a non-grinder's mouth of the same age. The damage compounds for years. Then a tooth that "should be fine" suddenly isn't.
The good news: grinding is one of the most controllable structural variables in dentistry.
A nightguard takes most of the spike off the teeth and onto the guard. Addressing bite imbalances stops asymmetric clenching that compensates for high spots. Treating sleep apnea (often associated with bruxism) sometimes reduces the grinding itself. None of these stop the habit entirely. All of them flatten the curve.
When a dentist asks about grinding even when nothing hurts, this is why. Catching it before fatigue makes it expensive is one of the highest-leverage moves in long-term dental care.
The Lesson
One idea. One lesson.
Every idea in the Structural Decision Framework gets its own lesson. Hover to feel the foil.
SDF-23
ForceGrinding and Fatigue Acceleration
Normal chewing is rhythmic and moderate. Grinding is a series of force spikes that overshoot what the tooth was built to absorb, and each spike adds microdamage. Over time, fatigue compounds and the tooth's ability to handle even normal forces drops.
↓ Open the model
Inside the Model
Read the diagram.
Through the Force lens, not all force is equal. Normal function is what teeth were designed for. Grinding isn't, and the difference between the two is what drives a lot of the structural decline that doesn't fit the patient's age, hygiene, or clinical history. Grinding and Fatigue Acceleration is the card that names the mechanism, so it can be addressed before fatigue makes it expensive.
Fig. 23 · Grinding and Fatigue Acceleration
SDF Framework
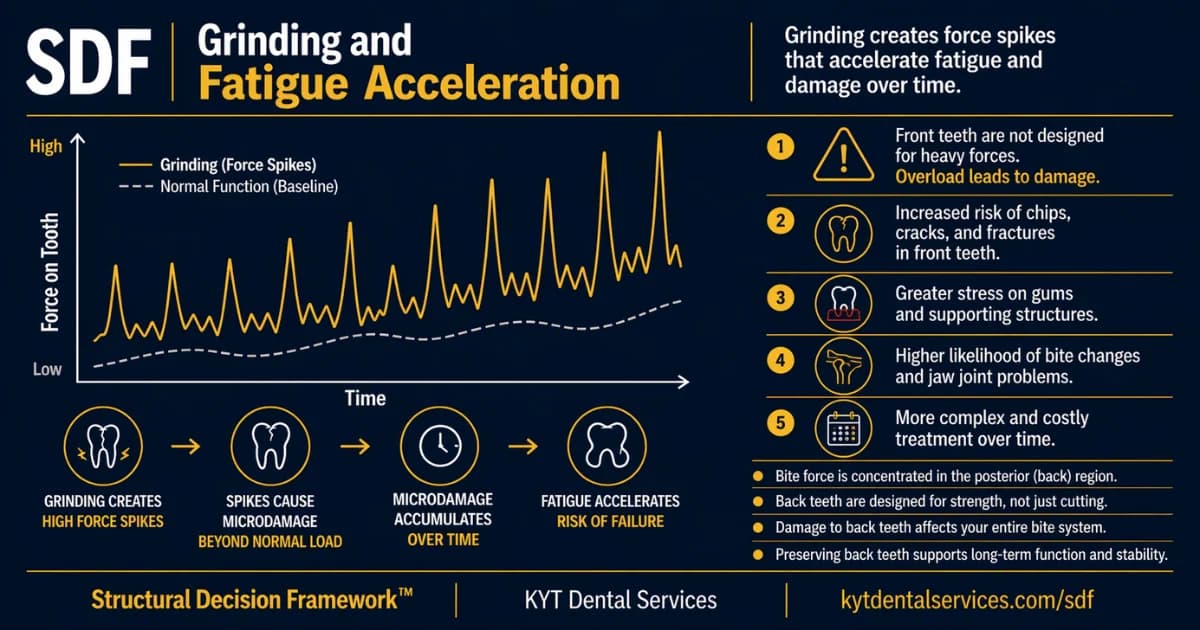
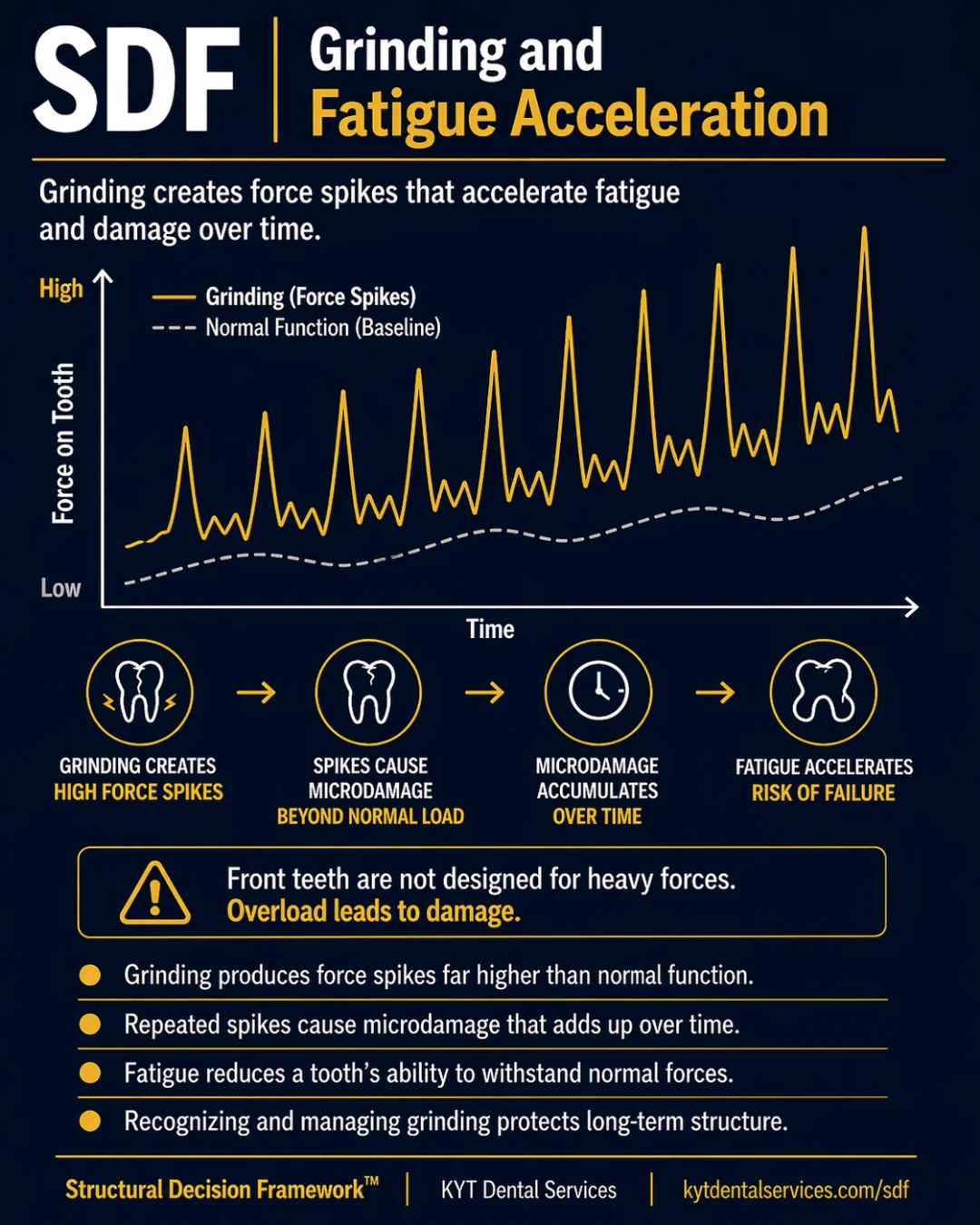
Normal chewing is moderate and rhythmic, well within what teeth were built to absorb. Grinding is a different kind of force entirely: spikes that overshoot the normal range, often at night, often unnoticed. Each spike adds microdamage that's invisible day-to-day but accumulates across years. Eventually, fatigue lowers the tooth's ability to handle even normal forces, and a tooth that 'should be fine' starts to fail. Managing grinding is one of the most controllable structural variables in dentistry.
Explanation
Teeth are designed for the kind of force they evolved to handle: chewing food, talking, swallowing, moderate, rhythmic, and within a predictable range. Grinding (bruxism) doesn't fit that pattern. It's force spikes, often two to ten times higher than normal chewing, often sustained for long periods, and most often happening during sleep when there's no conscious moderation. Each spike, on its own, doesn't break the tooth. What it does is leave a tiny amount of damage, a microcrack extension, a stress at a restoration margin, a flexure of a cusp. Microdamage accumulates the way fatigue does in any material: invisible until it isn't. The graph for a grinder doesn't look like a smooth line; it looks like spikes piled on top of a slowly rising baseline. Over years, two things happen at once. The microdamage adds up to visible structural problems, cracks, worn cusps, broken restorations, sensitivity. And the tooth's ability to absorb force drops, because the structure that used to spread the load isn't there to spread it anymore. The same chewing force that was routine ten years ago becomes a stress event today. That's how grinding accelerates the curve. The good news is that grinding is also one of the most controllable structural variables. Once it's recognized, a nightguard takes most of the spike off the teeth and onto the guard. Addressing bite issues, managing stress, and adjusting habits all flatten the curve. The earlier it's recognized, the less of the cumulative damage has to be undone with restoration.
Key takeaways
- Normal chewing forces are moderate and rhythmic, within the range teeth were built for.
- Grinding produces force spikes far above that range, often at night and often unnoticed.
- Each spike adds microdamage that's invisible day-to-day but compounds across years.
- Fatigue lowers a tooth's ability to handle even normal forces, making 'normal' chewing more damaging over time.
- Recognizing and managing grinding (nightguard, bite balance, habit awareness) is one of the most controllable structural moves available.
In the chair
How it shows up.
01
The 'why is this happening to me' tooth
A patient at 45 cracks a back tooth that's never been touched. They brush, they floss, they've never had a cavity on that tooth. The structural reason isn't decay, it's fatigue. Years of nighttime grinding produced enough cumulative microdamage to take a tooth that looked fine to the threshold. The crack wasn't sudden; the spikes had been adding up for two decades.
02
The nightguard that flattened the curve
A patient with multiple worn cusps and chipped front teeth gets a nightguard at age 38. Five years later, the wear has stopped progressing, the new restorations are intact, the front teeth haven't chipped further, and the joint pain that had been creeping up is gone. Nothing about the patient's grinding habit changed. What changed was where the force landed: on the guard, not the teeth.
03
The bite-balance fix
A patient comes in with sensitivity and unexplained wear on one side of the mouth. The exam shows the bite is uneven, the patient is unconsciously clenching harder on the high side to compensate. A bite adjustment redistributes the force; the wear pattern stops. The patient hadn't realized they were grinding because it was happening as compensation, not as a habit. Recognizing the cause flattened the curve without requiring nightly equipment.
Through other lenses
The same idea, three other ways.
The whole card is about force magnitude. Grinding isn't a different action, it's the same chewing motion at much higher load, applied repeatedly. The structural cost scales with the force, not the frequency.
Time is what turns grinding from 'a habit' into 'a structural problem.' One night of grinding doesn't show up. Twenty years of it does. The damage accumulates silently for the early years and visibly for the later ones, same mechanism, different point on the curve.
Each grinding spike costs structure, a microcrack growing a fraction of a millimeter, a restoration margin breaking down a little, a cusp flexing past its limit. None of these are visible day to day. All of them are what makes a grinder's mouth structurally older than a non-grinder's mouth of the same age.
Common questions
FAQ.
How do I know if I grind?+
Common signs: waking up with sore jaw muscles, headaches in the temples, sensitive teeth that have no obvious cause, worn-flat cusps, chipped front edges, or a partner who hears you grind at night. Most grinders don't realize they do it because it happens during sleep. A dentist can usually tell from wear patterns even before the patient is aware.
Is grinding the same as clenching?+
Both are forms of bruxism, but the force profile is slightly different. Grinding is lateral motion, teeth sliding against each other, which produces wear and shear forces. Clenching is sustained vertical force, squeezing without movement, which produces compressive load. Both create force spikes far above normal function and both contribute to fatigue. Many people do some of each.
Will a nightguard fix the problem?+
It won't stop the grinding habit, but it dramatically reduces the structural cost. The guard absorbs most of the force that would otherwise land on the teeth, and it spreads what does land more evenly. Most patients see the wear pattern stop progressing within months of consistent use. The guard wears out (because it's taking the damage), which is the point.
Can grinding be cured rather than managed?+
Sometimes the underlying cause can be addressed, bite imbalance corrected, stress managed, sleep apnea (which is associated with bruxism) treated. Those interventions can reduce or stop the grinding itself. But for most patients, grinding is a habit that comes and goes across life stages, so the structural protection (nightguard, regular monitoring) is the more reliable long-term move.
What's the most useful thing I can do if I grind?+
Three things, in order. First, get a nightguard fitted by your dentist, over-the-counter ones are better than nothing but don't fit well enough to do the job long-term. Second, address contributing factors: stress, caffeine, alcohol before bed, untreated sleep apnea. Third, build the structural protection into your dental decisions, when you do need restorations, choose ones that hold up under high force (full-coverage crowns over large fillings on grinders' molars, for example). Each one of these flattens the curve.
See this lesson in a real case
Stories behind this lesson.
Patient cases where this idea showed up in the chair.
See it in real teeth
From idea to actual cases.
This site explains the idea. The clinical version, with real cases, real X-rays, and what this looks like in actual mouths, lives at KYT Dental Services, the practice this framework comes from.
See it on KYT Dental Services →Keep going