Optionality Narrows Over Time
Lesson 19 · Structural Decision Framework
In plain English
We see this all the time: a patient asks why we treated their daughter's small cavity differently than we treated their own, same kind of tooth, same kind of finding, same family.
Their daughter's cavity, caught at age 30, had options: watch it, change diet to slow it, fluoride treatment, or place a small filling. The dentist and the patient picked from a wide menu.
The same kind of finding on the patient at 55, after years of skipped checkups, had two options: root canal plus crown, or extraction. Same kind of cavity. Different menus. Time was the variable that removed everything in between.
This is the part most patients don't realize:
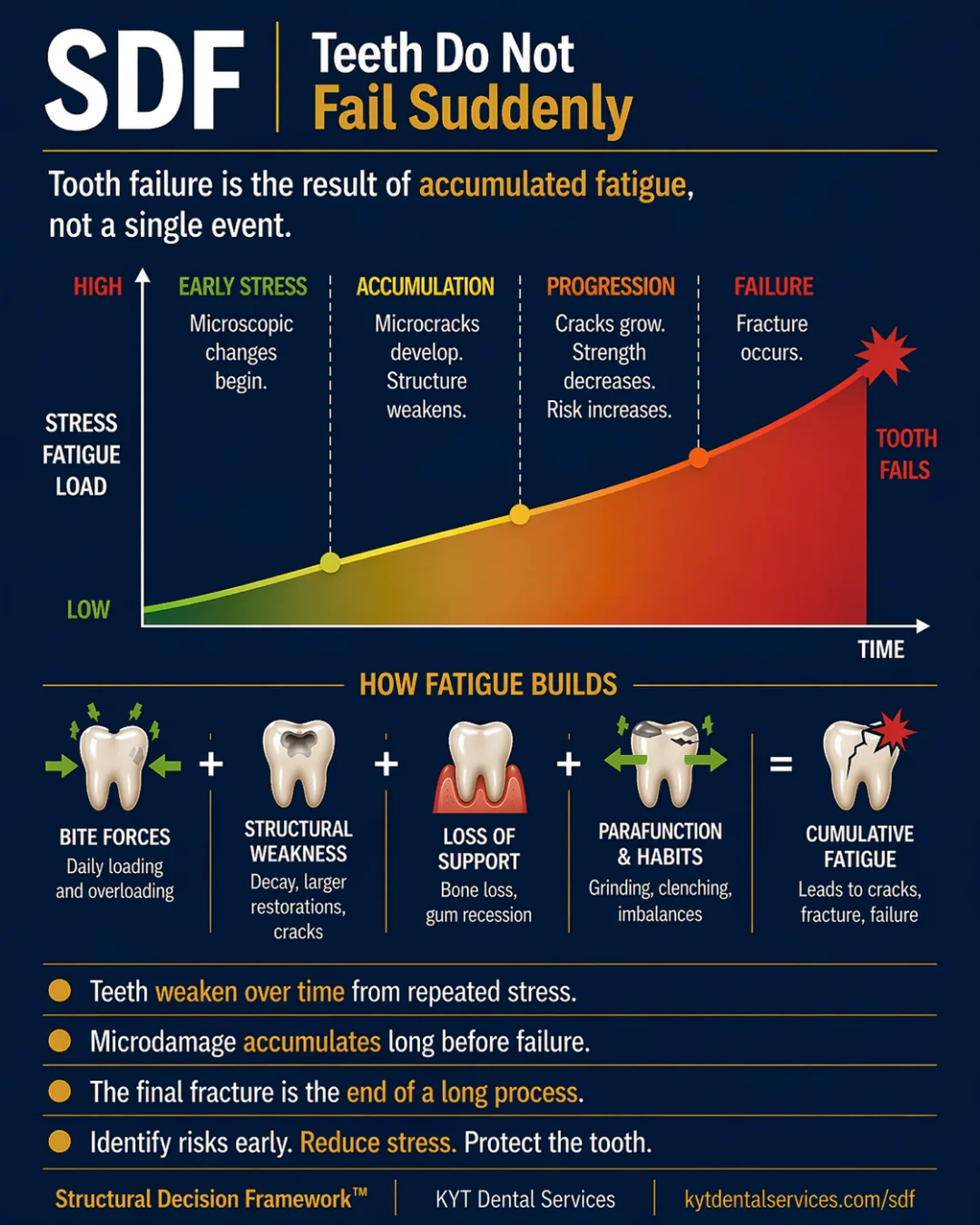
The choices available to a tooth aren't constant, they're a depleting set. The longer a finding goes uncaught and untreated, the fewer good options remain. The remaining options get more invasive and less reversible.
Three phases:
Early phase: full menu. Monitor and watch. Prevent (reduce force, change habits, address diet). Treat minimally, small filling, sealant, polished edge. Restore conservatively. Or do nothing and maintain. Most options preserve most of the tooth. The patient and dentist pick based on priorities, not because there's only one path.
Middle phase: simpler options have aged out. Monitor isn't enough, the problem is moving. Minimal treatment isn't enough, the damage is past where small fixes work. The remaining options are restoration, more complex treatment, and managing damage that has already happened.
Late phase: narrow menu. Extensive treatment (root canal plus crown, full coverage) or accepting tooth loss. None of the early options are still on the table.
Acting earlier isn't always about "fixing things faster." It's about keeping the menu wide. "Monitor and wait" is a real option in the early phase. It stops being one in the late phase. Time is what consumes the menu.
The patients who fare best across decades aren't the ones who treat everything aggressively or watch everything indefinitely. They're the ones whose findings stay in the early phase long enough that they always have choices.
The Lesson
One idea. One lesson.
Every idea in the Structural Decision Framework gets its own lesson. Hover to feel the foil.
SDF-19
TimeOptionality Narrows Over Time
Early on, almost every option is on the table. As damage progresses, choices fall off the menu. The longer you wait, the smaller the menu, and the more invasive what's left becomes.
↓ Open the model
Inside the Model
Read the diagram.
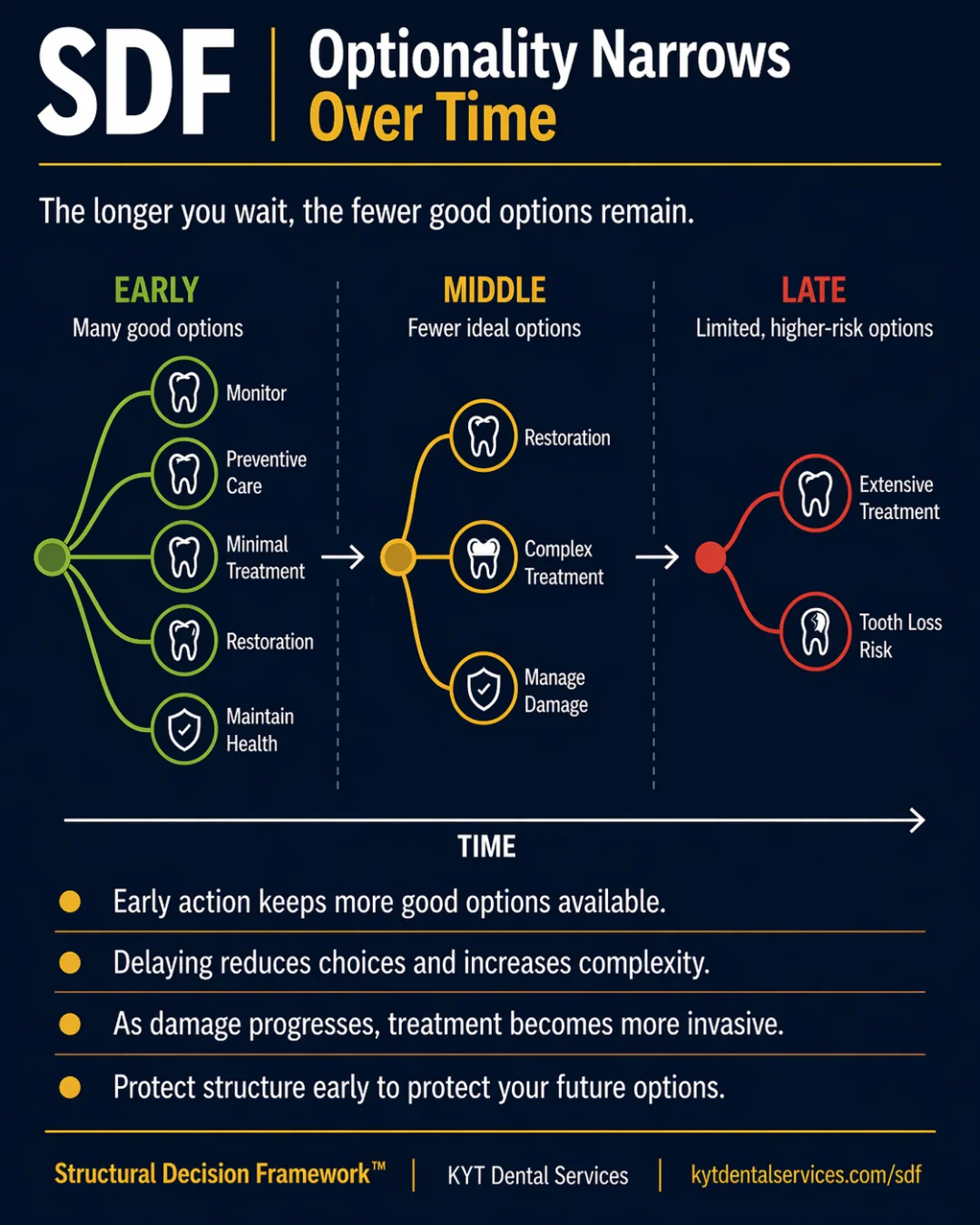
Through the Time lens, the choices available to a tooth aren't constant, they're a depleting set. Optionality Narrows Over Time is the card that makes that visible. The same finding has many possible answers in the early phase, fewer in the middle, and only a few in the late phase. Time itself is the thing removing options from the menu.
Fig. 19 · Optionality Narrows Over Time
SDF Framework
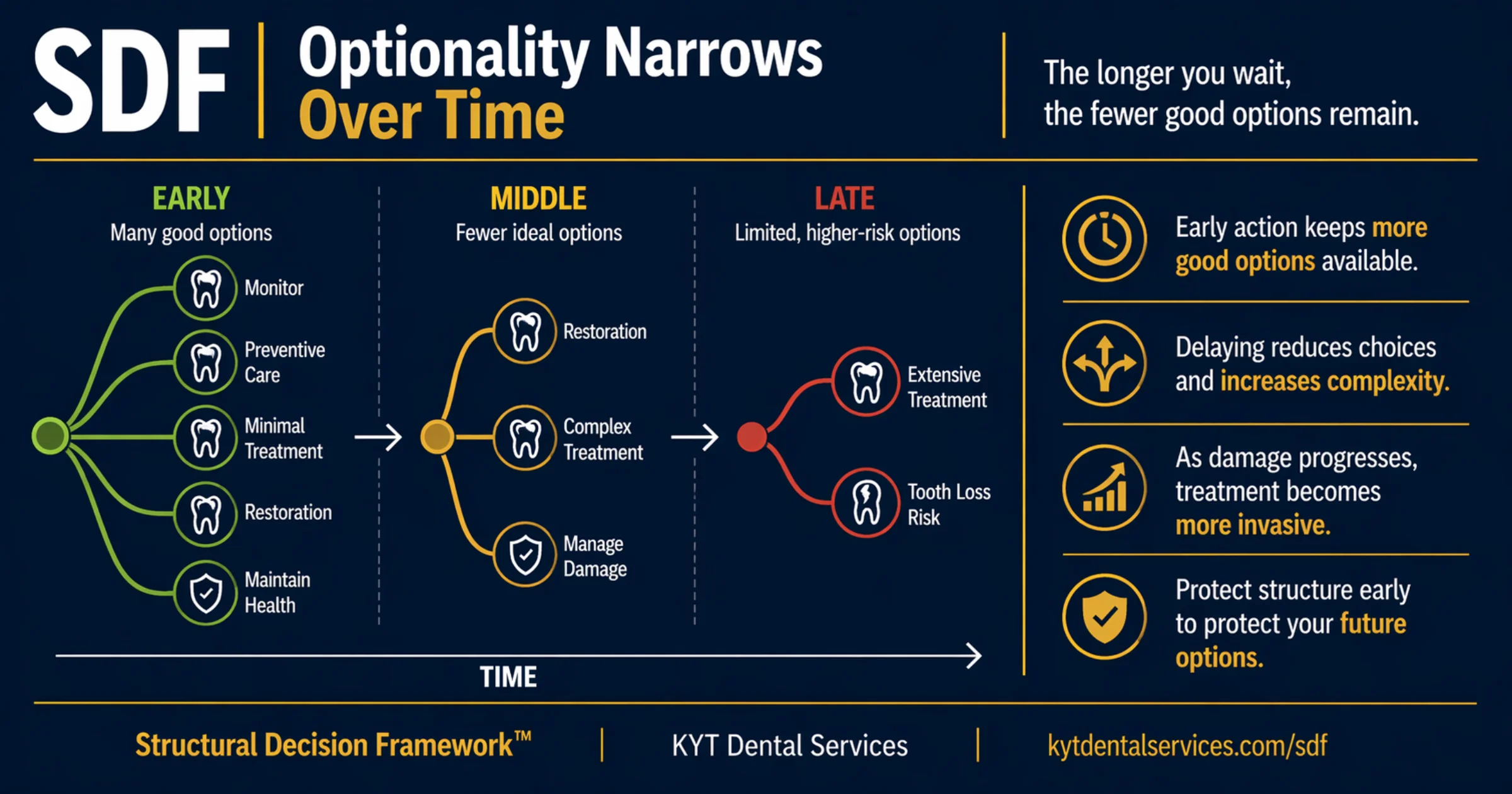
Every dental finding has a menu of possible responses, and the menu changes over time. Early on, when there's still plenty of structure and the problem hasn't progressed, almost every option is available, including 'do nothing for now and watch.' As damage accumulates, options fall off the menu one by one. By the time a finding reaches the late phase, the remaining choices are usually larger procedures with more cost, more recovery, and less reversibility. Optionality itself is something time consumes.
Explanation
It's tempting to think of a dental problem as one decision: either treat it or don't. The reality is that each finding sits inside a shrinking menu of possible responses. In the early phase, the menu is wide. You can monitor and see if it's stable. You can prevent (reduce force, address bite, change habits). You can treat minimally, a small filling, a sealant, a polished edge. You can restore conservatively. You can leave it alone and maintain. Most of these options preserve most of the tooth. In the middle phase, the simpler options have aged out. Monitoring isn't enough anymore, the problem is moving. Minimal treatment isn't enough, the damage is past where small fixes work. The remaining options are restoration, more complex treatment, and managing damage that has already happened. In the late phase, the menu is narrow. The choices are usually some version of extensive treatment (root canal, crown, full coverage) or accepting tooth loss. None of the early options are still on the table. The point of acting earlier rather than later isn't that early treatment is automatically better. It's that early action keeps the menu wide, so you have the choice of which path to take, instead of being handed the only one left.
Key takeaways
- Early on, the menu of options is at its widest, including 'monitor and wait.'
- Each stage of progression removes options from the menu.
- The remaining options become more invasive and less reversible the longer you wait.
- Acting in the early phase isn't always treatment, sometimes the right action is monitoring while the menu is still full.
- Protecting optionality is part of what early action accomplishes, it keeps you in control of the decision.
In the chair
How it shows up.
01
The early-phase menu
A small spot of decay shows up on a back tooth at age 35. The full menu is on the table, monitor it, change diet to slow it, treat with a small filling, treat with a different conservative approach. None of the options remove much structure. The patient and dentist can pick based on what fits their priorities, not because there's only one path. That's what an early-phase menu looks like.
02
The middle-phase narrowing
Five years later, the same kind of finding on a different tooth was missed at a couple of checkups. Now the decay is into the dentin and growing. Monitor isn't on the menu anymore. A small filling isn't enough. The choice is between a larger filling, a crown, or a more complex restoration. Each is more invasive than what would have worked five years ago. Each costs more structure today.
03
The late-phase decision
Another five years on, the same tooth comes back with deep decay reaching the nerve. The menu now has two real items: root canal plus crown, or extraction. Both are real treatments and both can be the right call, but neither is the conservative option that existed a decade ago. The decision is no smaller; the menu just is.
Through other lenses
The same idea, three other ways.
Time is what shrinks the menu. The same finding has different available options at different points on its curve. Reading the menu, what's still on it, what's already off it, is the timing skill that makes every dental decision better.
Each option that drops off the menu drops off because there isn't enough structure left to support it. Optionality and structure track each other, the more tooth is gone, the fewer responses fit. Preserving structure preserves choices.
Stability is what keeps the menu wide. A stable finding leaves all the early options viable for as long as the stability holds. The moment stability breaks, options start falling off, which is why catching the change matters more than treating immediately.
Common questions
FAQ.
If I have more options early, why don't dentists treat everything they find?+
Because 'wide menu' includes 'monitor and don't treat yet.' Early-phase findings often have no-treatment as a real option, and treating a stable finding too soon also costs structure. The point of a wide menu isn't that you must use the most active option on it; it's that you have the choice. Sometimes the best choice is to wait and watch.
How do I know which phase a finding is in?+
Your dentist can usually tell you. Specific signs include whether the finding is changing between visits, whether symptoms have started, how close it is to the nerve, and how much surrounding structure is intact. If the recommendation list still includes 'we could just watch this' as a real option, you're in the early phase. If 'watch' has dropped off, you're in the middle. If the conversation is mostly about which larger procedure to do, you're in the late phase.
Can the menu ever widen again?+
Sometimes, partially. Treatment can stabilize a tooth and put some options back on the table for the future. A crown can take a tooth from the late phase back into a more stable place. But the menu doesn't fully reset, because the structure that was lost doesn't come back. The new wider menu is wider than 'no menu,' but not as wide as the original.
What's the most useful thing I can do as a patient?+
Stay in the early phase. That's a combination of regular checkups (so findings are caught while the menu is still wide), addressing the things that drive progression (force, hygiene, diet), and being willing to act when the menu starts narrowing rather than waiting until you're forced to. None of those guarantee the menu stays wide forever. Together, they're how you keep more of it for longer.
Is the late phase always bad?+
Not always, late-phase treatment can still produce a tooth that lasts decades. But the cost is higher, the recovery is more involved, and the long-term outlook depends more on doing each remaining step well. The narrower the menu, the less margin for the next decision. That's why the framework treats optionality as something worth protecting on its own, not just as a side effect of preserving structure.
See this lesson in a real case
Stories behind this lesson.
Patient cases where this idea showed up in the chair.
See it in real teeth
From idea to actual cases.
This site explains the idea. The clinical version, with real cases, real X-rays, and what this looks like in actual mouths, lives at KYT Dental Services, the practice this framework comes from.
See it on KYT Dental Services →Keep going