The Fatigue Acceleration Curve
Lesson 16 · Structural Decision Framework
In plain English
We see this all the time: a hairline crack we've been watching for five years on a back tooth. Stable. No symptoms. Then in one six-month window, the crack reaches the nerve and the patient needs a root canal.
The patient is shocked. "It was fine for years."
It was. And then it wasn't. Nothing about the patient changed. What changed is where the crack was on the curve.
Here's the part most people don't realize about damage:
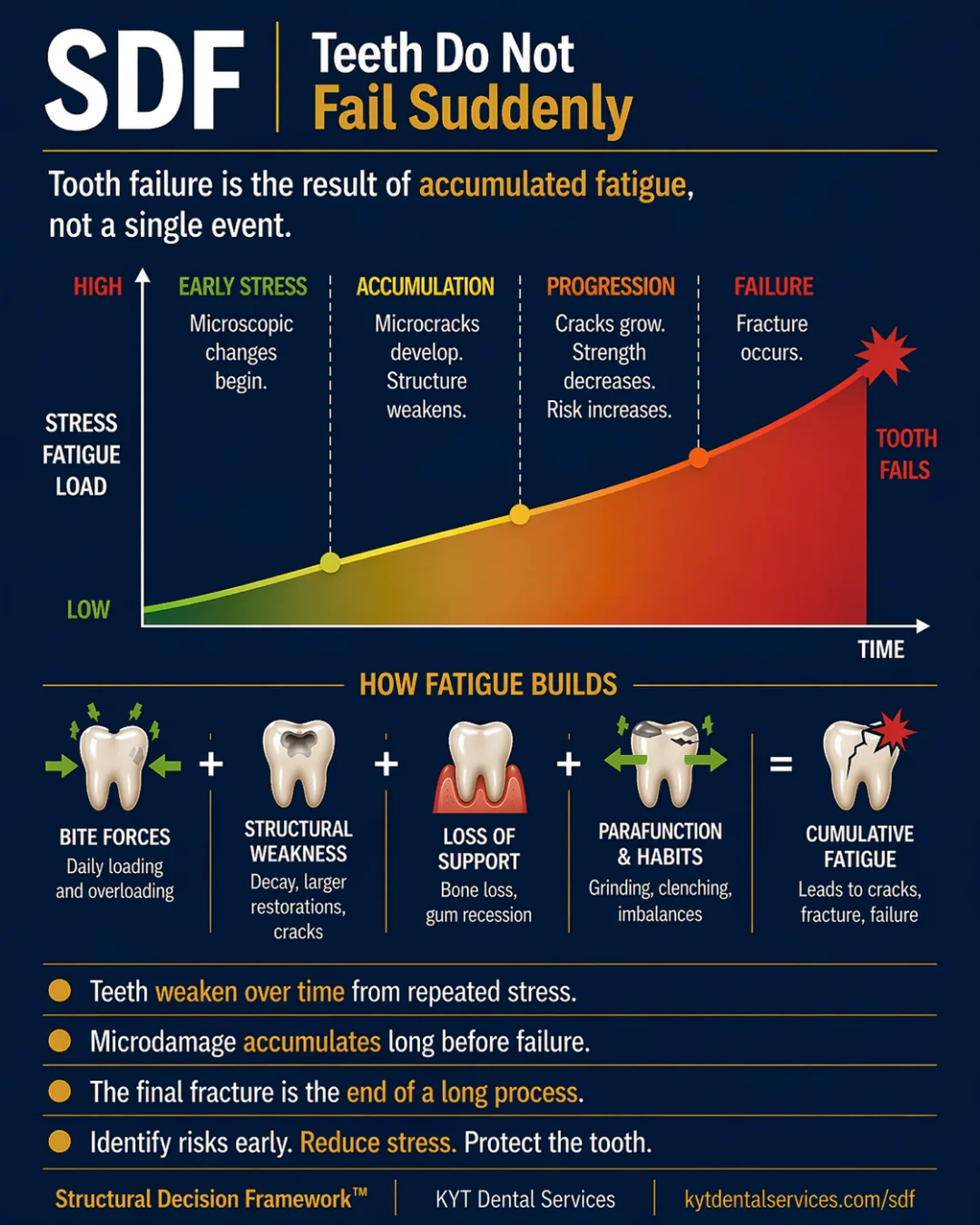
Damage to a tooth doesn't happen at a steady rate. It compounds. Small changes early stay small. Small changes late don't.
The curve isn't a slope, it's a swoop. Flat for a long time, then steep.
In the early phase, the tooth has its full structure. Cracks are microscopic. Loads are spread across plenty of material. Each year produces almost no measurable change. You could watch a finding here for years and see nothing.
In the middle phase, the changes are still small per year, but they're accumulating. Most aren't visible from the outside. The patient feels fine. The tooth still works.
Past the threshold, two things shift at once. The remaining structure has less material to absorb force, so each load does more damage. And the existing weaknesses concentrate stress on themselves, so they grow faster. The same input that produced a tiny change in year one now produces a visible problem in month one.
That's why a finding that's been "fine for years" can suddenly deteriorate dramatically. It's not the cause of damage that changed. It's the slope of the curve.
This is the math that makes early action so disproportionately powerful. The leverage of a small intervention isn't a matter of philosophy, it's the curve. A finding caught in the early phase stays small for a long time. The same finding caught past the threshold doesn't.
The Lesson
One idea. One lesson.
Every idea in the Structural Decision Framework gets its own lesson. Hover to feel the foil.
SDF-16
TimeThe Fatigue Acceleration Curve
Damage doesn't happen all at once, and it doesn't happen at a steady pace. It compounds. Small changes early stay small. Small changes late don't.
↓ Open the model
Inside the Model
Read the diagram.
Through the Time lens, the curve is the whole story. The Fatigue Acceleration Curve is the card that names its shape, flat early, steep late. Once you understand the curve, every other timing decision in dentistry makes sense: why monitoring matters, why pain is a late signal, why a 'sudden' fracture isn't actually sudden, and why the same finding has different right answers at different points in time.
Fig. 16 · The Fatigue Acceleration Curve
SDF Framework
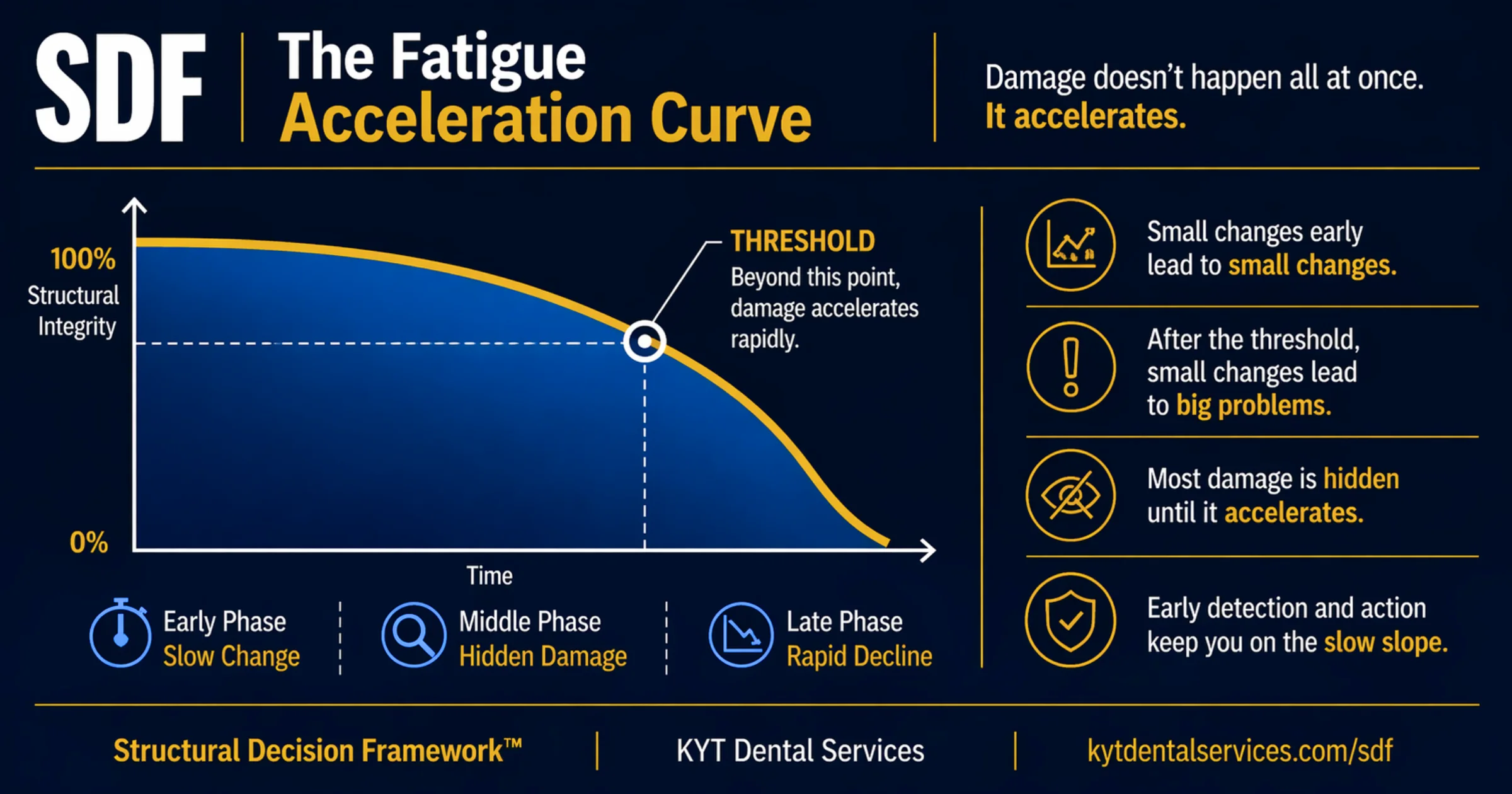
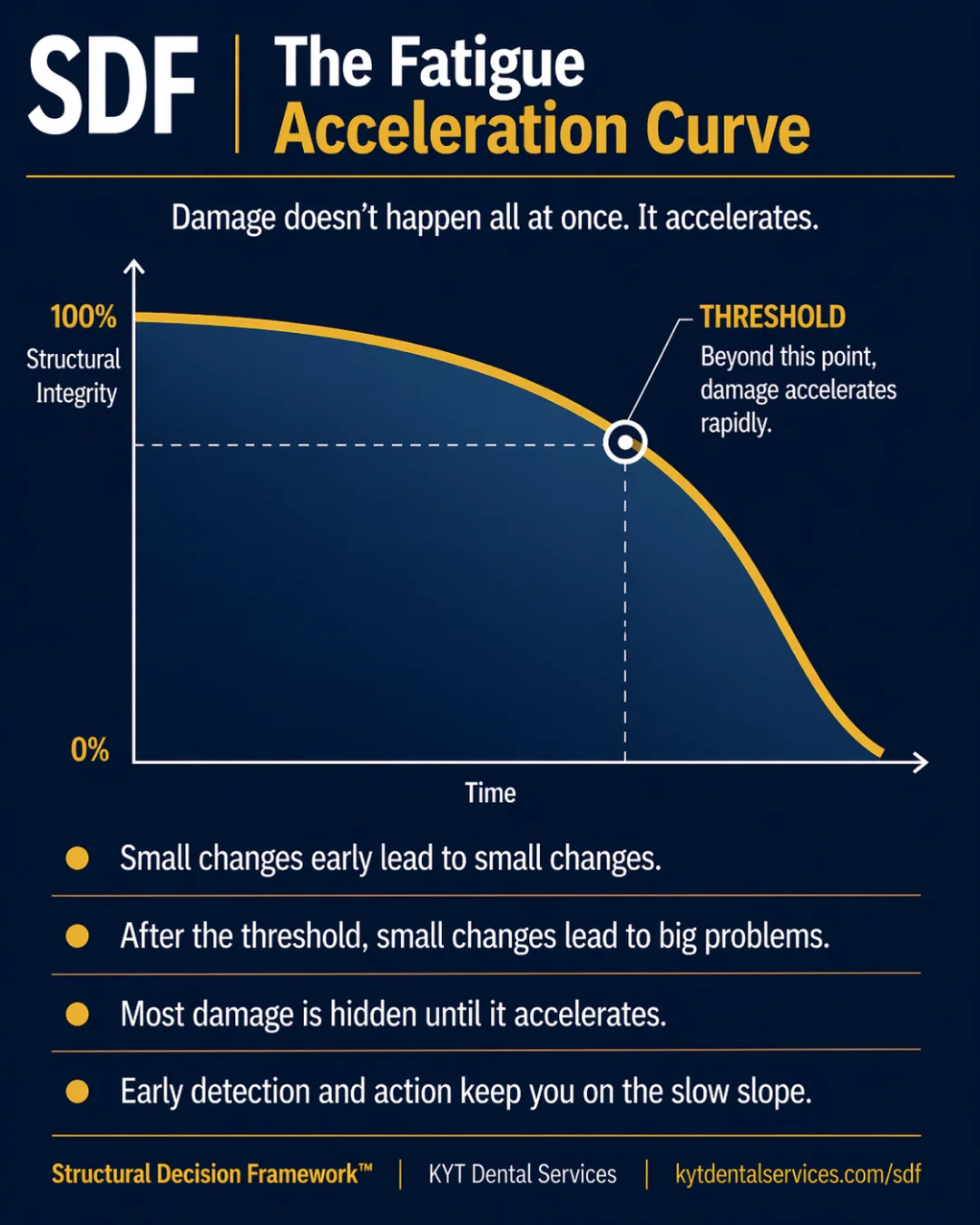
Tooth damage doesn't happen at a steady rate. It compounds. The early phase is slow and mostly silent. The middle phase hides changes that are accumulating. Past a threshold, the same small loads that took years to do anything start producing real damage in months. The curve is shaped like a swoop, flat for a long time, then steep. That shape is what makes early action so disproportionately high-leverage and late action so much more expensive.
Explanation
If damage were linear, the math of dentistry would be simple: every small loss is the same as the last one, and treating early or late wouldn't change much. Damage isn't linear. The early phase is slow because the tooth has its full structure, the cracks are microscopic, and the loads are spread across plenty of material. The middle phase is the deceptive one, changes are still small per year, but they're accumulating, and most of them aren't visible from the outside. Past the threshold, two things shift at once. The remaining structure has less material to absorb force, so each load does more damage. And the existing changes, small cracks, weakened cusps, exposed dentin, concentrate stress on themselves, so they grow faster. The same input that produced a tiny change in year one now produces a visible problem in month one. That's why a finding that's been 'fine for years' can deteriorate dramatically in a relatively short time once it crosses the threshold. It's not the cause of damage that changed. It's the slope of the curve.
Key takeaways
- Small changes early lead to small changes, the curve is flat for a long time.
- Past the threshold, small changes lead to big problems, the same input now does more damage.
- Most damage is hidden until it accelerates, patients usually feel the late phase, not the early one.
- Early detection and action keep you on the slow slope, where each year costs less structure.
- The shape of the curve is why early intervention has so much more leverage than late intervention.
In the chair
How it shows up.
01
The five-year-old crack that wasn't
A patient has a hairline crack noted at every checkup for five years. No symptoms, no growth. Then in one six-month window, the crack reaches the nerve and the tooth needs a root canal. Nothing about the patient's habits changed. What changed was where the crack was on the curve, the years of slow growth had reached the threshold, and the next stretch was steep.
02
The cleaning that prevented the curve
A patient had early-stage gum disease at age 40, caught at a routine checkup. Regular cleanings and at-home care kept it in the slow phase indefinitely. At 60, they still had the same baseline. The early phase didn't end, because the inputs that would have driven it past the threshold were managed.
03
The cliff after pain
A patient with no dental pain for years suddenly has constant pain in one tooth. By the time they get to the dentist, the X-ray shows what looks like decades of slow change followed by a recent acceleration. The pain didn't start the damage, it started when the tooth crossed the threshold. The 'sudden' problem was a long curve catching up.
Through other lenses
The same idea, three other ways.
Time is what moves a tooth along the curve. The curve doesn't change shape; the tooth's position on it does. Reading where on the curve each tooth sits, and how fast it's moving, is the timing skill that makes every other dental decision better.
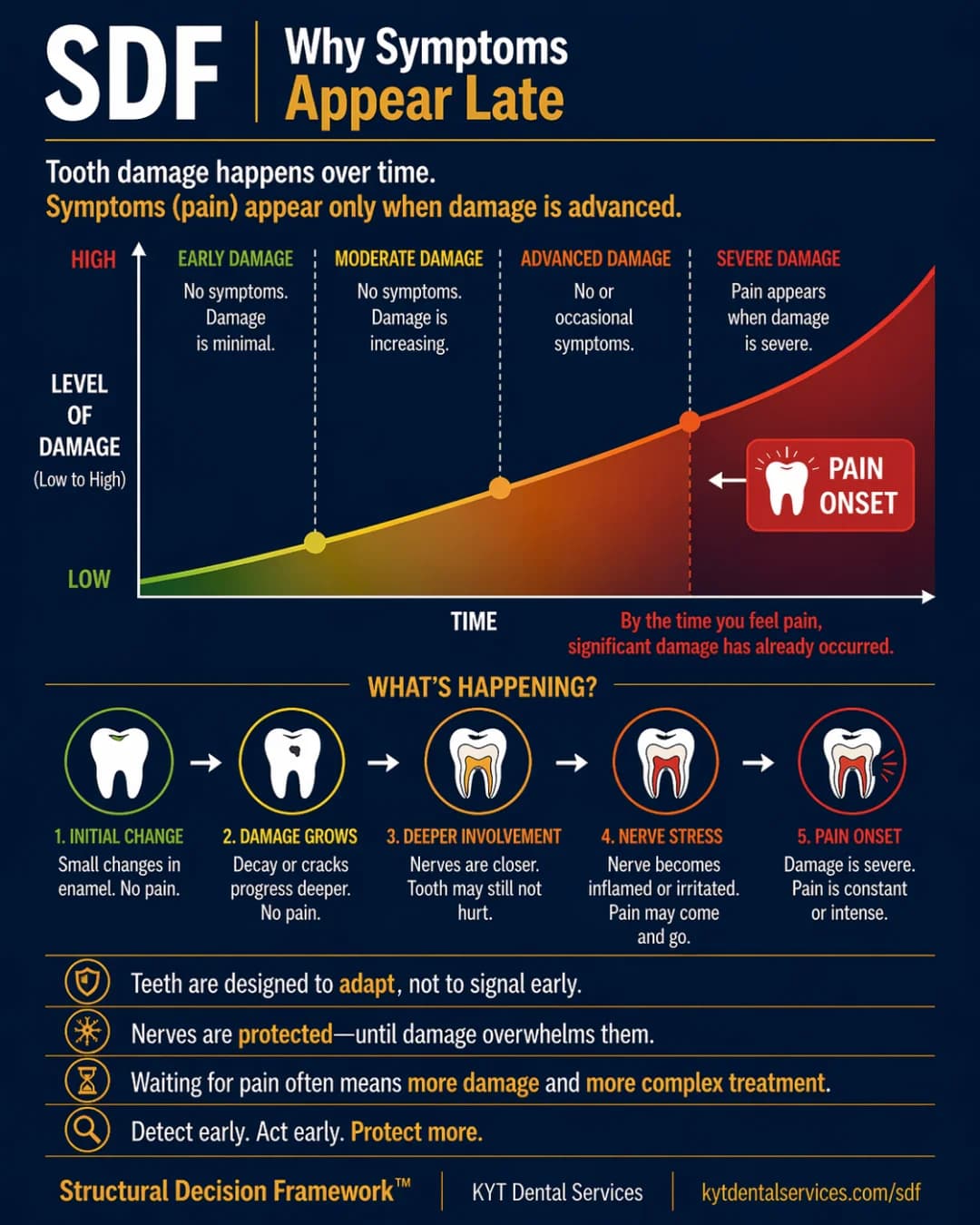
The curve is a structural curve. It tracks how much of the tooth is still doing structural work, not whether it hurts. Structure can be deep into decline before any symptoms show up, which is why the early and middle phases are mostly silent.
Force is what drives the tooth along the curve. Higher forces move it faster. Lower forces (after a nightguard, a bite adjustment, or addressing grinding) flatten the slope. You can't change the shape of the curve, but you can change how fast a tooth travels along it.
Common questions
FAQ.
Why doesn't damage happen at a steady rate?+
Because the tooth absorbs damage differently at different stages. With full structure, force is spread across plenty of material and small changes barely register. As structure is lost, the same force is concentrated on less material, and existing weaknesses (cracks, exposed dentin, cusps under stress) magnify each new load. The slope steepens because the tooth's ability to absorb damage drops faster than the damage rate itself.
Can a tooth go from 'fine' to 'in trouble' that fast?+
Once it crosses the threshold, yes. The 'fine for years' phase isn't really fine, it's the early/middle phase where damage was building silently. The 'sudden' decline is the curve doing what it always does past the threshold. Patients experience it as fast because they were only feeling the late phase.
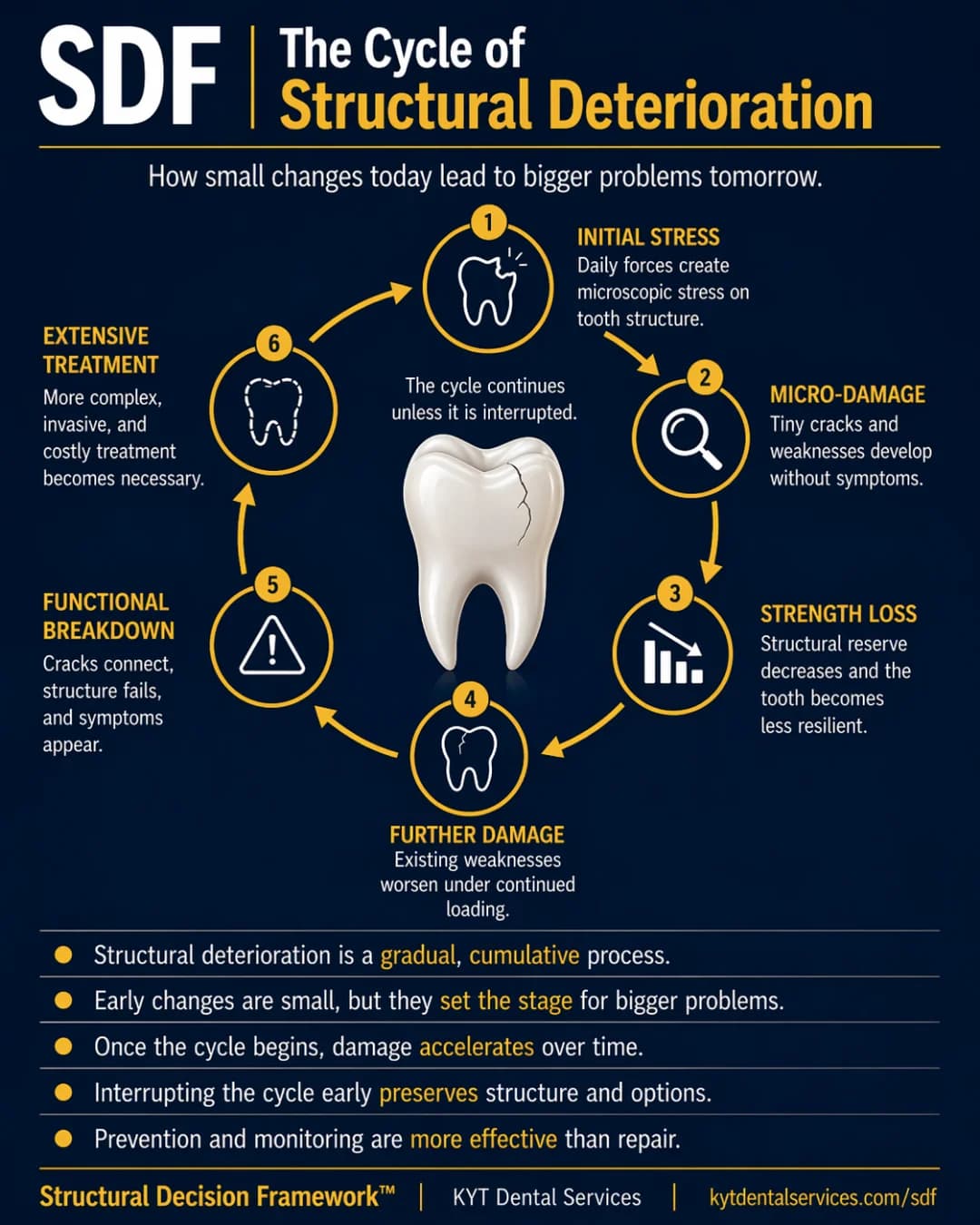
Can the curve be reset?+
Sometimes, partially. Restorations, crowns, and gum treatments can rebuild some of the structure or stability that was lost, which effectively moves a tooth back along the curve. But the natural tooth structure that's gone is gone. The reset is partial, which is why preventing the slide in the first place is more effective than reversing it.
How do dentists know where on the curve a tooth is?+
By looking at the structural reads (X-ray, exam), the rate of change between visits, and the symptoms (or lack of them). Two teeth with the same current condition can be in different phases, one is stable in the early phase, one is just before the threshold. The trajectory matters more than the snapshot, which is why baseline records and consistent monitoring are valuable.
What's the most useful thing I can do as a patient?+
Stay on the slow slope. That's a combination of regular checkups (so changes are caught early), addressing forces you can control (grinding, bite issues, hard-chewing habits), and treating findings while they're still in the stability window. None of those slow the curve dramatically on their own. Together, they're how a tooth stays in the early phase for decades instead of years.
See this lesson in a real case
The story behind this lesson.
A patient case where this idea showed up in the chair.
See it in real teeth
From idea to actual cases.
This site explains the idea. The clinical version, with real cases, real X-rays, and what this looks like in actual mouths, lives at KYT Dental Services, the practice this framework comes from.
See it on KYT Dental Services →Keep going