Acting Too Soon vs Acting Too Late
Lesson 15 · Structural Decision Framework
In plain English
We see this all the time: two patients with the same exact finding, a small spot of decay confined to the enamel, get completely different treatments at completely different times.
Patient A came in nervous. "I want to fix it now, even if it's small." The filling went in. Healthy structure was removed to make room for it. Five years later, the matching tooth on the other side, same kind of spot, never treated, still hadn't progressed. The treated tooth had permanently lost structure to fix something that wasn't going anywhere.
Patient B skipped checkups for three years. By the time they came in, the same kind of spot had grown into the dentin, gotten close to the nerve, and now needed a root canal plus a crown.
Same finding. Two timing errors. Two structurally costly outcomes.
Here's the part most patients don't realize:
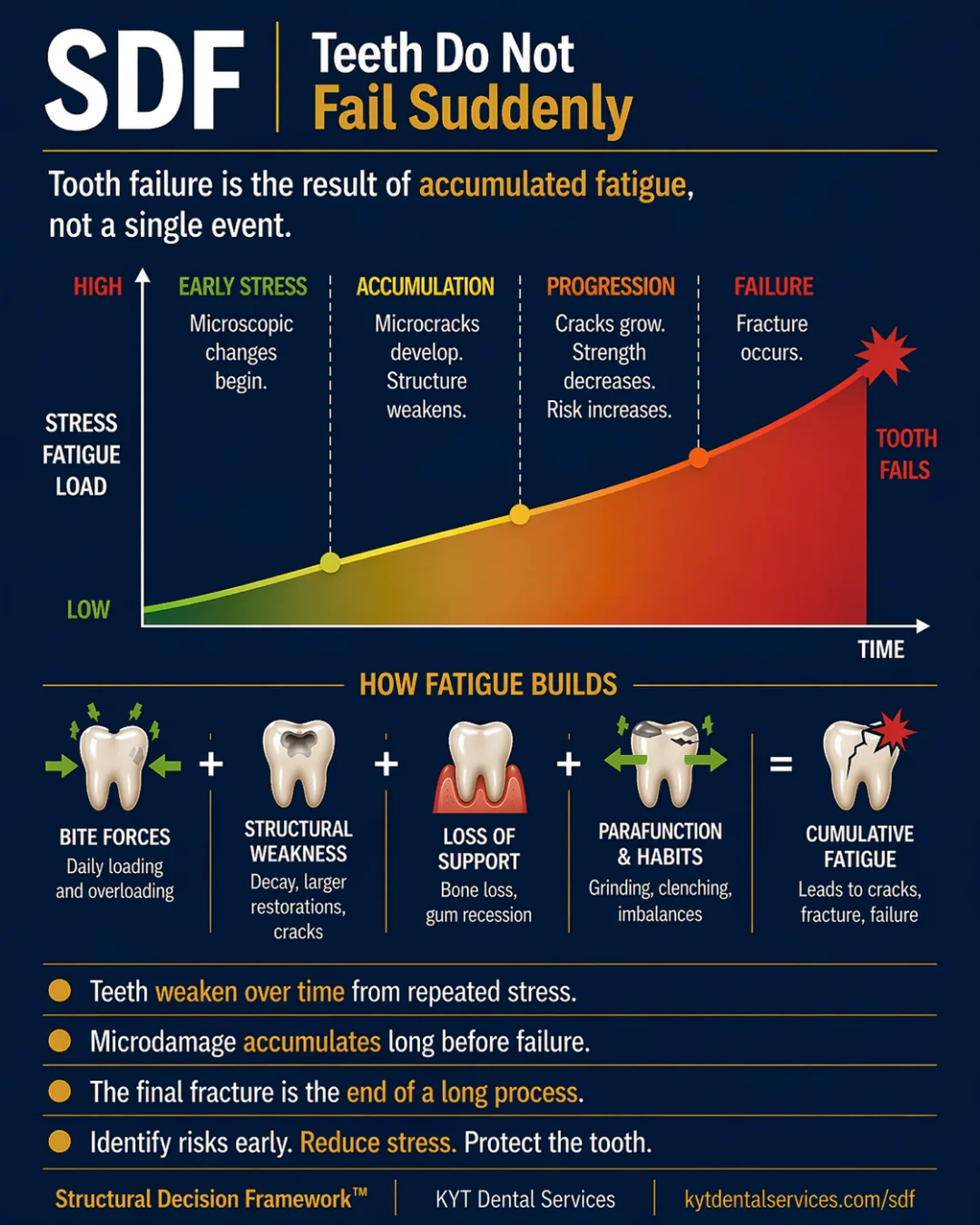
Bad timing in dentistry costs structure in both directions.
Acting too soon = removing healthy tooth structure for a problem that wasn't actually progressing. The finding was stable. The procedure was real. The structure that's gone doesn't come back.
Acting too late = letting the finding cross the threshold where small interventions stop being enough. Same finding, bigger procedure, more structure lost.
The right time is in the middle, when risk is rising but structure is still mostly intact. "Earlier is always better" isn't true when earlier means "before it was needed." "Watch and wait" isn't true when waiting means "past the point of no return."
The hardest skill in dentistry isn't doing the procedure. It's reading the curve and acting at the moment risk is rising, not the earliest possible moment, and not after the curve has turned.
The Lesson
One idea. One lesson.
Every idea in the Structural Decision Framework gets its own lesson. Hover to feel the foil.
SDF-15
TimeActing Too Soon vs Acting Too Late
Bad timing costs structure in both directions. Acting too early removes healthy tooth. Acting too late lets damage cross the threshold. The goal is the right time, not the safest one.
↓ Open the model
Inside the Model
Read the diagram.
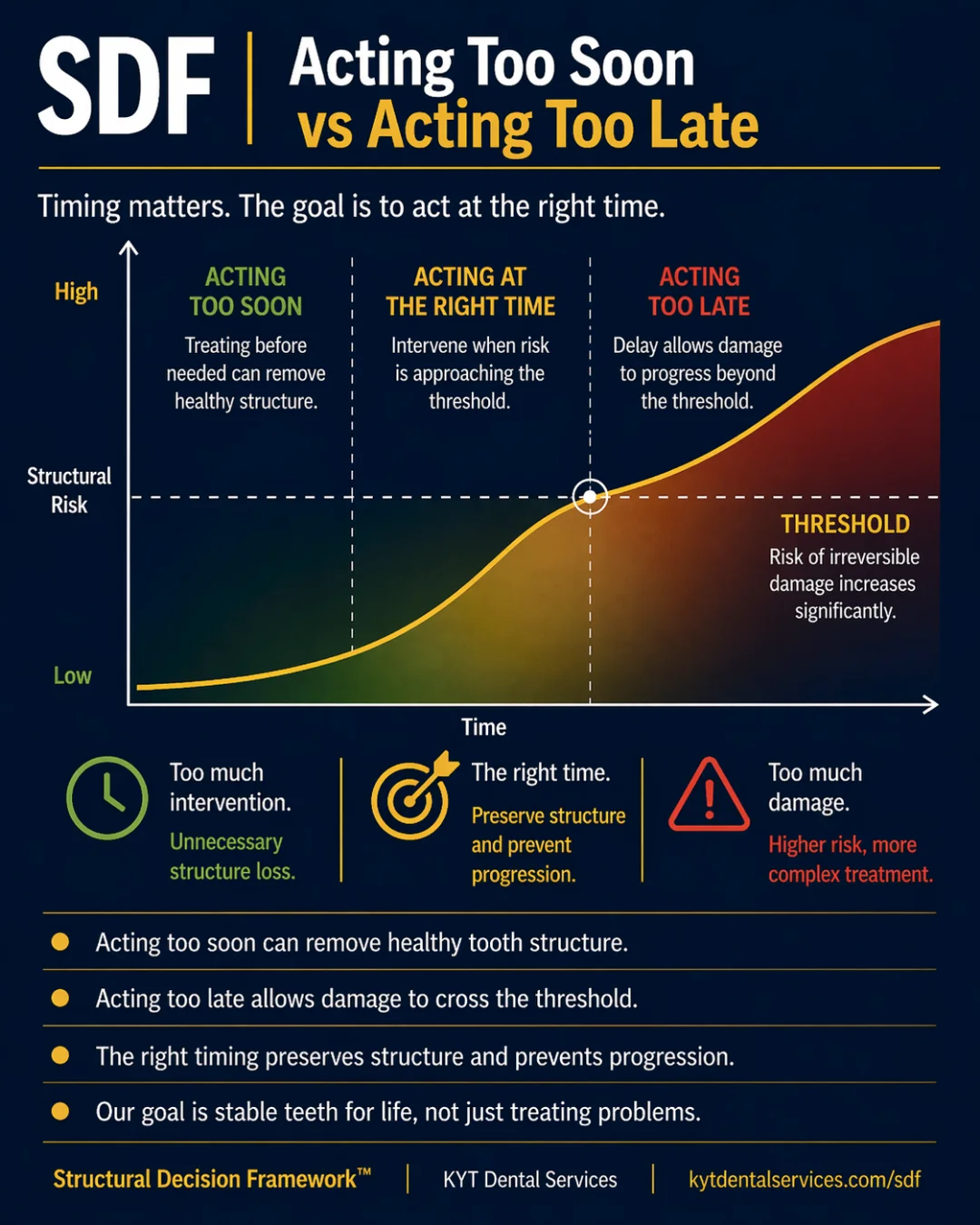
Through the Time lens, every finding sits on a curve, and every curve has a right moment to act on it. Acting Too Soon vs Acting Too Late is the card that names both errors. Treating early costs structure that didn't need to go. Treating late costs structure that could have been saved. Both come from misreading where the tooth is on its curve.
Fig. 15 · Acting Too Soon vs Acting Too Late
SDF Framework

Timing is the variable that decides how much structure a treatment costs. Acting too soon removes healthy tooth for a problem that wasn't actually progressing. Acting too late lets the problem cross the threshold where small interventions stop being enough. The goal isn't the earliest treatment or the latest, it's the right time, when risk is approaching the threshold and the response can still be small.
Explanation
Most dental problems sit on a curve where structural risk rises slowly, then accelerates. The same problem treated at three different points on that curve has three very different costs. Treated too early, the problem may not have needed treating at all, and the procedure removed healthy structure that wasn't actually at risk. Treated at the right time, when risk is rising but hasn't yet hit the threshold, the procedure is small and the structure is mostly preserved. Treated too late, after the threshold, the problem has accelerated. The procedure is bigger, the structure remaining is smaller, and the chance of needing future work on the same tooth goes up. Both errors, too soon and too late, cost structure. They just come at it from opposite directions. The skill of timing isn't about being aggressive or conservative as a default. It's about reading where each tooth is on its curve, and acting when the curve is about to turn.
Key takeaways
- Acting too soon can remove healthy tooth structure for a problem that wasn't progressing.
- Acting too late allows damage to cross the threshold and forces a more aggressive procedure.
- The right timing preserves structure and prevents progression, both errors cost more.
- Regular monitoring is what makes the right timing possible, you can't catch the curve turning if you're not watching it.
- The goal is stable teeth for life, not the most or least dentistry.
In the chair
How it shows up.
01
The early intervention that wasn't needed
A small enamel-only spot on a back tooth gets filled at the first visit. Two years later, the patient learns that the same kind of spot on the matching tooth, left alone, never progressed. The treated tooth permanently lost healthy structure to fix something that wasn't going anywhere. The intent was conservative; the timing made it the opposite.
02
The right-time crown
A patient has a tooth with a moderate crack and increasing chewing sensitivity. The dentist watched it for a year, then placed a crown when the symptom started rising. The crack didn't reach the nerve. The tooth kept its structure under the crown. The timing was the win, earlier would have been overtreatment; later would have meant a root canal.
03
The waited-too-long extraction
A patient skipped checkups for years. By the time they came in for pain, the tooth that needed a crown two years ago now needed extraction. The same finding, at two different times on the curve, has two different answers. Time alone, unmonitored, is what made the difference.
Through other lenses
The same idea, three other ways.
Time is the whole card. The same finding has different right answers at different points on its curve. The skill of timing is reading the curve, not picking a posture (aggressive or conservative) and applying it everywhere.
Both errors cost structure. Too soon costs healthy structure that didn't need to go. Too late costs structure that could have been saved with a smaller procedure. The right time is the timing that preserves the most tooth across the whole life of the tooth.
Stability is what good timing buys. A tooth treated at the right moment stays stable longer than the same tooth treated early or late. The goal isn't the procedure; it's the trajectory the procedure puts the tooth on.
Common questions
FAQ.
How can treating something early be wrong?+
Because every procedure has a structural cost. Filling, crowning, or treating a tooth removes some healthy tissue along with whatever is being treated. If the original finding wasn't going to progress, that cost was paid for nothing. The healthy tooth structure that's gone doesn't come back. 'Earlier is always better' isn't true when earlier means 'before it was needed.'
How do I know if my dentist is recommending treatment too soon?+
Ask what the alternative is and what would happen if you waited. A reasonable answer sounds like 'this is approaching the threshold and waiting risks crossing it' or 'we've watched this for X months and it's changing.' A weaker answer is 'we should fix everything we find.' If the recommendation can't be tied to a specific change or risk, it's worth slowing down.
How do I know if I'm waiting too long?+
Listen to the symptoms and watch the trajectory. New chewing sensitivity, a finding that grew between visits, or a recommendation that's now bigger than it was before are all signs the curve is turning. A finding that was 'monitor' last visit and is now 'treat' is doing exactly what the framework predicts, and acting at that point keeps it from sliding further.
Is the right time the same for every patient?+
No. The same finding on two different teeth in two different mouths can have different right times, depending on how much structure is left, how much force the tooth takes, and how the patient's other teeth are trending. The skill is patient-specific timing, not a universal rule.
Can the right time be 'never'?+
Yes. Some findings are genuinely stable across decades and never need treatment. Monitoring is the right answer for those, and watching them prove out as stable is part of how the framework works. 'Never' is a real outcome, not a delay.
See this lesson in a real case
Stories behind this lesson.
Patient cases where this idea showed up in the chair.
See it in real teeth
From idea to actual cases.
This site explains the idea. The clinical version, with real cases, real X-rays, and what this looks like in actual mouths, lives at KYT Dental Services, the practice this framework comes from.
See it on KYT Dental Services →Keep going